Antimicrobial Resistance, Host‑Directed Therapy, and the CCR5 Pathway
Geoffrey Fourqurean, Neuroscientist and Patient Advocate, Independent Consultant
Antimicrobial resistance (AMR) threatens millions worldwide, yet mortality often stems as much from immune dysregulation as from pathogen load. Lessons from COVID 19 demonstrate that host directed therapies, such as CCR5 blockade to reduce RANTES driven cytokine storms, may complement traditional antibiotics. Integrating pathogen and host focused strategies could reshape the global response to AMR and improve survival outcomes.
Global Burden of AMR
The World Health Organization projects that resistant infections could claim up to ten million lives annually by 2050 if urgent action is not taken. This looming crisis is not only a microbiological challenge but also a public‑health, economic, and geopolitical threat. Developing countries, especially across Africa and Asia, face disproportionate risk because of limited laboratory capacity, shortages of trained personnel, gaps in antibiotic stewardship, and higher baseline burdens of infectious disease. Beyond mortality, AMR undermines modern medicine itself. Surgeries, cancer chemotherapy, neonatal intensive care, and organ transplantation all depend on reliable prophylaxis and treatment. When first‑line agents fail, clinicians must fall back to toxic or expensive second‑line drugs, lengthening hospital stays and driving poor outcomes. Families shoulder catastrophic costs from repeated admissions, while health systems absorb productivity losses as patients recover more slowly or not at all. The World Bank estimates cumulative global GDP losses in the trillions if resistance trends continue, a drag comparable to the 2008 financial crisis but smoldering rather than explosive. Behind the projections is a simple truth: every resistant infection is a race between pathogen growth and host resilience, and in too many cases the host loses.
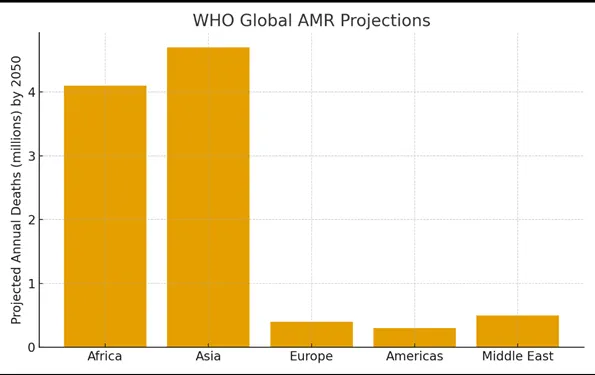
Figure 1. WHO Global AMR Projections (projected annual deaths by 2050). Source: WHO, 2019.
Why Host‑Directed Therapy Belongs in AMR
Antibiotics act on microbes; patients die from the combined effects of microbe and dysregulated host response. In pneumonia, sepsis, and many drug‑resistant infections, tissue injury accelerates when chemokines recruit large numbers of activated immune cells into already stressed organs. CCR5, the receptor for CCL5/RANTES, CCL3/MIP‑1α, and CCL4/MIP‑1β, coordinates this traffic. Excess signaling pushes macrophages and effector T cells into inflamed lungs, liver, and brain, amplifying cytokine loops and microvascular leak. Modulating CCR5 does not replace antibiotics; it reduces collateral damage so pathogen clearance and organ recovery can proceed. Conceptually, this is the core of host‑directed therapy: alter the terrain upon which the battle is fought, not only the enemy itself.
Mechanism Snapshot: CCR5/RANTES
CCR5 is expressed on memory T cells, monocytes/macrophages, dendritic cells, and microglia. Ligand engagement triggers G‑protein signaling that drives chemotaxis, adhesion, and activation. In acute lung injury and sepsis, persistent CCR5 signaling sustains leukocyte recruitment and endothelial activation, elevating IL‑6 and TNF, disrupting barrier integrity, and worsening hypoxemia. Antagonism of CCR5 can blunt these cascades: leukocyte trafficking falls, NF‑κB activation diminishes, and inflammatory mediators decline. Clinically meaningful biomarkers consistent with benefit include restoration of the CD4:CD8 ratio, decreasing IL‑6, improved PaO2/FiO2, falling vasopressor requirements, and reductions in CRP and ferritin. Human genetics underscores the pathway’s importance: individuals homozygous for the CCR5‑Δ32 mutation are highly resistant to HIV infection, and heterozygotes often show altered susceptibility to severe infectious disease.
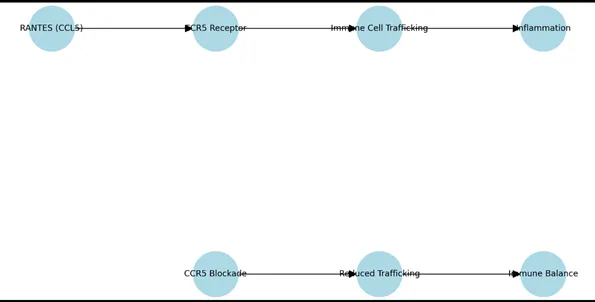
Figure 2a–b. CCR5/RANTES pathway (top) and CCR5 blockade restoring balance (bottom). Schematic.
Clinical Lessons from COVID‑19
COVID‑19 crystallized the point that inflammation can become lethal even as replication wanes. Across small but consistent datasets, CCR5 antagonism was associated with reductions in IL‑6, movement of lymphocyte subsets toward homeostasis, and survival trends in the sickest cohorts. These signals do not, by themselves, solve AMR. They do provide a translational bridge: when hyperinflammation magnifies risk, targeted immunomodulation can be lifesaving alongside pathogen‑directed care. Similar dynamics arise in severe influenza, secondary bacterial pneumonias, and some fungal diseases, strengthening the case that CCR5 modulation is a platform strategy rather than a niche fix.
A Dual Strategy Against AMR
Pairing antibiotics with CCR5 antagonism is conceptually simple, kill the organism, calm the storm, but operational success requires discipline. Patient selection should rely on objective markers of hyperinflammation (e.g., IL‑6, CRP, ferritin, D‑dimer) and clinical deterioration despite appropriate antimicrobial therapy and source control. Timing matters: immunomodulation should begin as organ dysfunction emerges, not after multiorgan failure has taken hold. In practice, dual therapy could allow shorter or lower‑dose antibiotic courses, reduce ventilator and vasopressor days, and prevent the spiral toward refractory shock. Because host‑directed agents act on conserved human pathways, they retain relevance even as pathogen landscapes shift or new resistance mechanisms appear.
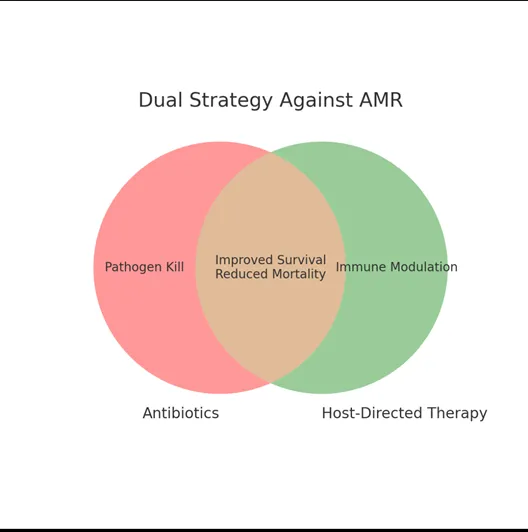
Figure 3. Dual strategy: Antibiotics (pathogen kill) + host‑directed therapy (immune modulation).
Hospital Implementation Pathways
Health systems can pilot a host‑plus‑pathogen protocol inside existing antimicrobial stewardship programs. A workable framework includes five steps. Step 1: Eligibility screening on admission and daily thereafter, focusing on suspected or confirmed infection with rising oxygen needs, escalating pressors, or encephalopathy plus inflammatory biomarker elevation. Step 2: Early multidisciplinary consult (critical care, infectious disease, pharmacy) to verify that antibiotics and source control are optimized. Step 3: Initiate CCR5 antagonism under protocol with baseline labs and predefined safety checks. Step 4: Track outcomes that matter, ventilator‑free days, vasopressor‑free days, renal‑replacement‑free days, total ICU length of stay, survival, and record antibiotic days of therapy to quantify stewardship impact. Step 5: Monthly review by a stewardship committee to refine inclusion criteria, dosing, and stop rules, and to publish outcomes transparently whether positive or negative.
Evidence Beyond COVID‑19
Outside respiratory pandemics, dysregulated inflammation drives mortality in bacterial sepsis, certain parasitic infections, and invasive fungal disease. Across preclinical models, blocking CCR5 reduces leukocyte infiltration, edema, and capillary leak, with downstream improvements in gas exchange and organ function. Observational human data, such as altered infection trajectories among CCR5‑Δ32 carriers, support a causal role for the pathway. These strands justify hospital‑level pilots with careful pharmacovigilance while randomized trials are organized. Critically, host‑directed agents can be started even when the organism has not yet been identified, a window during which inappropriate empiric therapy often accumulates and resistance risk rises.
Diagnostics and Biomarkers for Selection
Success depends on choosing the right patient at the right time. Universal cytokine testing is unrealistic, so a tiered approach is pragmatic. Hospitals without IL‑6 should begin with CRP and neutrophil‑to‑lymphocyte ratio trends coupled to bedside indicators such as rising FiO2 or escalating norepinephrine. Where IL‑6 is available, thresholds and trajectories can refine timing. Protocolized flowsheets ensure decisions are consistent across shifts and clinicians, minimizing subjective bias.
Health‑Economic Case
ICU care is the most expensive real estate in a hospital. Even a one‑day reduction in organ‑support requirements yields substantial savings that can exceed the price of an immunomodulator. When shorter antibiotic courses are feasible, downstream costs fall further, fewer cases of Clostridioides difficile, less nephrotoxicity, and fewer resistant breakthrough infections. Administrators respond to numbers: a simple dashboard comparing pre‑ and post‑implementation trends in ICU length of stay, antibiotic days of therapy, and survival will drive adoption faster than theory alone.
Equity, Ethics, and Safety
Host‑directed therapy must never delay antibiotics or source control. Patient selection should exclude profound neutropenia without active marrow recovery and uncontrolled opportunistic infection. Protocols for low‑ and middle‑income settings should emphasize bedside criteria and low‑cost labs, with clear stop‑rules to avoid over‑immunosuppression. Equity also means access: pooled procurement and tiered pricing can prevent a two‑tier world in which only wealthy systems can implement modern AMR care.
Illustrative Case (Hypothetical)
A 63‑year‑old man with diabetes is admitted with culture‑positive, ventilated Klebsiella pneumonia. Despite appropriate carbapenem therapy and drainage of a small pleural collection, his oxygenation worsens and vasopressors escalate. IL‑6 and CRP are markedly elevated; lymphocytes are suppressed. Under the hospital’s host‑plus‑pathogen protocol, a CCR5 antagonist is added. Over 48 hours, FiO2 falls, norepinephrine is weaned, and the patient transitions to a spontaneous breathing trial by day five. Antibiotics are completed in eight days without relapse. While anecdotal, this arc illustrates how immunomodulation can unlock recovery once the infectious source is controlled and highlights measurable endpoints—organ‑support‑free days and total antibiotic exposure.
Limitations and Counterarguments
Skeptics rightly note that not all inflammation is harmful and that dampening immune traffic might blunt microbial clearance. That is why patient selection and timing are paramount: use host‑directed therapy for documented hyperinflammation tied to organ dysfunction, and never as a substitute for antibiotics or source control. Another concern is generalizability, signals from viral ARDS do not guarantee benefit in every resistant bacteremia. The correct response is disciplined trials, transparent reporting, and a willingness to stop or pivot if outcomes do not improve. Learning fast, and honestly, is the responsible path forward.
Research Roadmap
Near‑term studies can be launched without large grants. First, a prospective registry capturing all patients treated under a CCR5‑augmented protocol, including eligibility criteria, biomarkers, timing, dosing, and outcomes. Second, a pragmatic randomized pilot comparing standard of care versus standard plus CCR5 antagonism in hyperinflammatory phenotypes, powered for ventilator‑free days with survival as a key secondary endpoint. Third, a pharmacovigilance analysis focused on hepatic events and secondary infections, with 90‑day follow‑up. Standardized data dictionaries and open reporting will accelerate learning across sites. As signals clarify, multicenter trials can evaluate specific AMR syndromes, such as ventilated MDR pneumonia or complicated intra‑abdominal infection, with endpoints that integrate patient‑centered outcomes and antibiotic stewardship metrics. Regulatory dialogue should begin early so that positive pilots can translate into labeled indications or clear, ethically governed pathways for use.
Outlook
AMR is two problems braided together: evolving microbes and fragile hosts. The first demands better antibiotics; the second demands smarter immunology. Integrating CCR5 antagonism into stewardship‑anchored care pathways is a tractable near‑term experiment for health systems. The hypothesis is pragmatic: fewer deaths, fewer ICU days, and fewer antibiotic exposure days. That is a win that matters to patients and to hospitals alike, and it is achievable with protocols that are careful, measurable, and transparent. Looking forward, health systems should view host‑directed therapy not as an exotic adjunct but as the next evolution of evidence‑based critical care. By building pragmatic pilots, collecting rigorous safety and outcome data, and sharing results openly across networks, hospitals can move the field from theory to accepted practice. International collaboration is especially critical: pathogens and resistance do not respect borders, and lessons learned in one ICU can save lives in another continent. Ultimately, integrating immunology into antimicrobial stewardship is not just good medicine, it is global health security.
References
- World Health Organization. No Time to Wait: Securing the Future from Drug Resistant Infections. WHO; 2019.
- Seethamraju H, Smith DM, et al. CCR5 blockade in patients with severe COVID 19 treated with leronlimab: a case series. J Transl Autoimmun. 2021;4:100103.
- Yang OO, Pasikhova Y, et al. CCR5 blockade with leronlimab restores immune homeostasis in critical COVID 19. Clin Infect Dis. 2022;74(7):1180–1183.

Geoffrey Fourqurean is a neuroscientist and patient advocate with experience in immunology, infectious disease, and host-directed therapies. He writes about global health, HIV cure strategies, and antimicrobial resistance.

