The Use of Artificial Intelligence for Healthcare Improvement in Low-And Middle-Income Countries
Rudrajit Paul, Consultant Physician, Ruby General Hospital
Meera Suresh, Associate Professor, Department of Homeopathy, Lincoln University College
Artificial intelligence will be a boon in resource limited LMICs health sector especially in disease surveillance and policy making. The lag period evident during Covid mitigation responses exposed the existing lacunae and the necessity of such advanced technology in the health system. However, it requires appropriate training and research investment.
Introduction
Artificial Intelligence (AI) is an umbrella term which has been described in different ways. In its simplest form, AI is the science and engineering of making intelligent interconnected programs and computer systems which can simulate some aspects of human cognitive function and help in problem solving1.
In the medical setting, such cognitive technologies and machine learning algorithms may be used in a lot of ways including, but not limited to, disease surveillance, policy making and clinical work. Especially in low- and middle-income countries (LMIC) like India, where the human resources are limited, such AI based applications will lead to a paradigm shift in healthcare, both at personal and public health level, in the near future. In this article, some of the potential uses of AI in transformation of healthcare in LMIC will be discussed.
Disease surveillance:
The recent Covid pandemic has made the importance of disease surveillance painfully clear. In many regions, the early days of the pandemic were wasted in labor intensive data collection and analysis2. Had this time been better utilized, many initial outbreaks could have been prevented. For example, had the surveillance been timely in the initial quarter of 2021, the ravages of the second covid wave in April 2021 in India could have been prevented3.
Disease surveillance is an essential part of any health system. However, with time, the whole process of big data collection, analysis and dissemination is becoming too cumbersome for human enterprise. There are real life examples of successful use of AI for disease surveillance. For example, in 2009, during the Flu pandemic, such an international online database was maintained by the WHO which led to better coordination of global public health response4. More recently, Twitter based AI algorithm was used to detect possible Hantavirus outbreaks in Chile5. In Korea, such deep learning methods have been used successfully to predict public outbreaks of diseases like Scarlet fever and Malaria5.
Unless timely surveillance data is available, effective health policies can’t be devised. Using such AI based method also reduces the lag time of the reports. Even under best circumstances, epidemic reports prepared by medical societies or government departments have a significant delay of several weeks6. AI based systems can reduce the time lag considerably and this can mean more lives saved.
So, such machine learning is a feasible option in predicting some disease outbreaks in LMIC. However, in many regions of India, people still lack access to the internet. This will leave significant gaps in the data. Current internet penetration in India stands at around 50%7. But as more people are connected to the internet in the future, the sensitivity of the system will increase.
Epidemic intelligence:
Epidemic intelligence is defined as the whole process of systematic collection, analysis and interpretation of data related to disease outbreaks for purposes of timely public health response8. With the availability of big data, epidemic intelligence is becoming an important tool in public health9. The system utilizes two types of data: indicator based and event-based9. AI can help in quick collection of indicator-based data, as shown in figure 1.
Figure 1: Hypothetical framework for indicator-based data analysis (as proposed by Sathish Kumar et al)10 EMR: electronic medical records
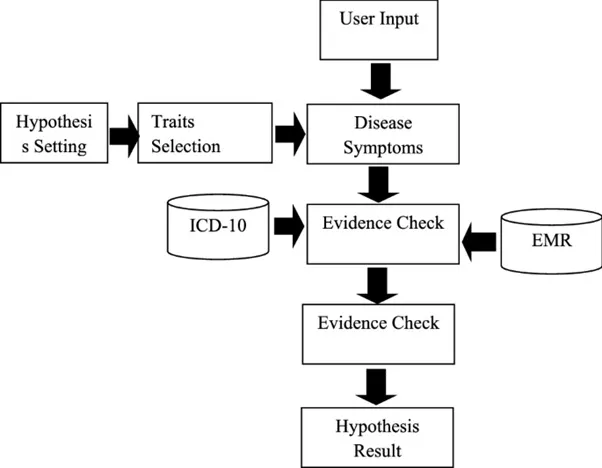
Of course, this model depends on correct data input at user level. Such electronic data is still scarce in countries like India. But with government sponsored pan-country medical insurance programs like Ayushman Bharat with their attendant digitized record keeping, such usable data will soon be generated.
In an innovative approach, combination of public health data with zoonotic surveillance data is also being tried11. With better connectivity, multiple geo-referenced and time series data are now combined by algorithms9. The Medi+ Board is such an innovative system where public health data from multiple sources are combined in real time11. These AI based systems are not only useful for detecting disease outbreak, but also for getting an early idea about public perception e.g. vaccine hesitancy12. Nyawa et al from France have recently shown that social media analysis using deep learning can effectively detect the trends in vaccine hesitancy. India is the country with the largest number of Facebook users worldwide. Thus, such social media-based health surveillance can be highly effective in India.
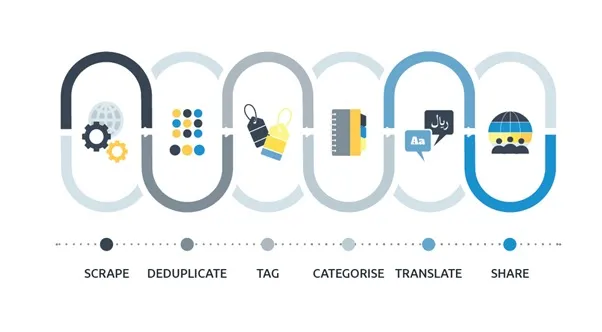
Recently, the WHO has also devised the EIOS system: Epidemic Intelligence from Open Sources13. This is a fit-for-purpose constantly evolving web-based system built as a part of public health initiative (PHI) activities13. This AI based system collates big data from multiple sources including news sites, blogs, expert groups, government health department sites and academic discussion boards. The data is then categorized, processed and published continuously. The scope of the system is shown in fig. 2. This data may be used for quick public health response in LMIC.
Figure 2: EIOS system of WHO for epidemic intelligence (https://www.who.int/initiatives/eios/eios-technology)
Personalized precision medicine:
The healthcare delivery system is slowly moving towards a patient-centered model of care14. This is especially true for chronic diseases. In LMIC like India, non-communicable diseases (NCD) like diabetes are rising in prevalence. It is estimated that out of total diabetics in the world, 80% live in LMIC15. But comprehensive treatment coverage is pathetically low in these regions15. AI can help in fulfilling these unmet needs to a great extent.
Increasing capture and digitization of data is helping healthcare organizations in improving service for chronic patients and reducing cost14. India has recently launched the National Programme for Prevention & Control of Cancer, Diabetes, and Cardiovascular Diseases & Stroke (NPCDCS). Neural network-based algorithms can be used to quickly assess the operational effectiveness of the programs and make predictions about at-risk patients14. Organizational management of such vertical programs in populous countries like India can also be vastly improved by neural network based learning16.
One recent example of the successful application of AI in disease care pathway was the diabetic retinopathy screening program in Zambia17. Here, AI based algorithm was able to successfully identify progressive diabetic retinopathy and also referable diabetic macular edema with sensitivity exceeding 95%17. In this project, the retinal images were captured by non-medically trained technicians17. Such a model may also be used in other LMIC, especially in regions with low access to human expertise. Intelligent medical devices with high diagnostic accuracy has also been marketed recently. One example is the IDx-DR device for diagnosis of retinopathy. This device uses AI to detect retinopathy in primary care even without help from ophthalmologist18.
Diagnostic assistance:
A new branch of medical diagnostics, that is being developed at fast pace, is radiomics. Machine learning (ML) may be used for predicting the diagnosis from radiological imaging data19. This may be especially helpful for early detection of cancer19. Such deep learning methods have already been used for successful detection of head-neck and lung cancers19. Recently, some models are being developed which can not only help in early cancer detection from radiological images, but also may predict survival.
Innovative approaches like combining FDG-PET and MRI images are also being tried to predict the probability of metastasis in certain types of cancer20. In many LMIC, radiologists are extremely scarce21. For example, as of 2018, Bangladesh had 4.3 radiologists per million population21. Thus, reporting is likely to be delayed and this leads to delay in initiation of cancer treatment. In such cases, AI based radiomics can help in cancer care. Many hospitals of India are now installing the PACS program for quicker analysis of radiology images22.
The other example of AI based clinical support is in diabetes. Data captured from continuous or intermittent manual glucose monitoring is sent to a cloud server which then uses ML to determine the insulin dose. A clinical trial has shown that using AI for determining insulin dose was non-inferior to specialist mediated dose adjustment23. This is another technology which may be used in LMIC effectively. Not only does this help in dose adjustment, but also this technology may be used to predict hypoglycemia24. In 2018, a smartphone application was developed, connected to the continuous glucose monitoring device, which can give warning one hour prior to probable hypoglycemia24. This can help patients to a large extent and prevent major clinical events.
Finally, for LMIC, another application of AI is in cardiology. LMICs have a lot of gaps in the care continuum of cardiology patients, stemming from multiple factors like lack of human resources and financial constraints25. One major application is in the early detection of arrhythmia25. Recently AI-based ECG systems have been developed that can detect arrhythmias ranging from atrial fibrillation to ventricular tachycardia with high degree of accuracy25. In countries like India, most healthcare settings do not have 24-hour cardiology expert support. Thus, most cardiac emergencies will be initially managed by nurses and primary care physicians. In such cases, such ML-based algorithms can help in better cardiac care. A recent study from Bangalore, India showed that the use of AI-powered mobile devices in the community can lead to earlier detection of structural heart diseases26. Such application of technology can help in better coverage of cardiac services.
ML based algorithms can revolutionize trauma care. In many LMIC, critical care specialists are extremely scarce and those available are mostly concentrated in specialized centres27. This makes trauma care at the rural level inadequate. In such cases, the use of AI can help fill the care gap to a large extent. Recently, AI has been used successfully to predict critical issues like pelvic hematoma and cervical spine injury in acute trauma settings28. Also, remote triage algorithms have been developed, which can stratify the level of care for incoming trauma patients28.
Health research:
AI can be used for biomedical research in LMIC. Large scale biomedical research is often difficult in LMIC due to cost factor and lack of industry support. However, without local normative data, effective policy making often remains incomplete. However, the use of ML can reduce the cost and time of research in many cases. For example, ML can be used to analyse large datasets like Genomic data quickly to understand the dynamics of infectious diseases29. Also, AI can be used for drug discovery and development30. In epidemiology, AI can be used for historical data analysis in retrospective studies.
The process of drug discovery can be sped up significantly if neural network is used. Many LMIC lack the technology necessary for large scale biochemical processing. But AI can bridge that technology gap virtually. All stages of drug development can be expedited, as shown in fig. 3 below.
Figure 3: The use of AI in drug development (Paul et al. available online from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7577280/ )
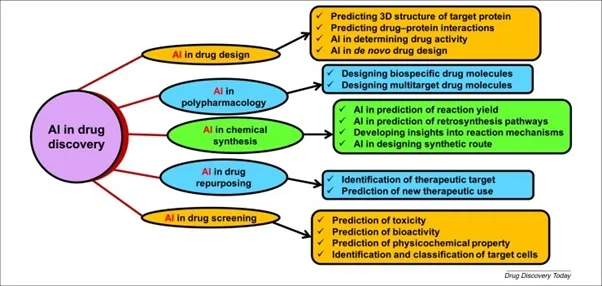
The development of virtual chemical space with virtual screen compounds and molecular fingerprint recognition technology has reduced the cost of new drug discovery significantly30. This is especially useful for emerging infectious diseases, which mostly affect LMICs. Deep neural network algorithms can help in prediction of physico-chemical properties, in vivo activity and toxicity of new molecules effectively31.
Digital twin:
The concept of health digital twins (HDT) has only recently gained acceptance and it has the potential to revolutionize personal healthcare32. In simplest terms, HDT is the virtual representation of a patient that is generated from multimodal patient data along with real time update on patient and environmental variables32. The HDT technology, which combines AI with Internet of Things (IOT) can even be used to measure and predict a patient’s response to medications on a case-to-case basis. In future, this may be used even to populate the control arms of large clinical trials32. The HDT model may even be used at the population level for public health programs as was shown recently in predicting and optimizing patient flow in certain hospitals in South Korea33. In LMIC, the distribution of healthcare facilities is often skewed and this technology may help in better utilization of healthcare resources. The market for digital twins is growing at an astronomical rate in the current decade34. However, this technology still has a lot of ethical and regulatory issues to solve.
Addressing environmental determinants of health:
In the current era of climate change, human health is intimately linked to environmental factors. AI can be used effectively in that area also. We know that air pollution is one of the main factors behind a lot of acute and chronic diseases like asthma, cardiovascular disease and cancer. AI can be used to accurately measure and predict air quality in a locale35. It can also suggest remedial measures like temporary shutting down of industries and decreasing traffic flow35. As is widely known, most of the highly polluted urban centres are located in LMIC36. These countries can use AI to reduce the impact of air pollution in the population. Many countries like China have already started a centralized plan for “intelligent environment protection” using AI37. A recent study from Nigeria has shown that AI can similarly be used to predict environmental water quality, which will have direct impact on food production and disease outbreaks38.
Conclusion:
Artificial intelligence is transforming healthcare in irreversible ways all over the world. LMICs can use the technology effectively in order to expand the healthcare access and bring about better equity while reducing wastage at the same time. However, for this model to be successful, there is need of training in appropriate technology and investment in research.
References: -
1. McCarthy J. What Is Artificial Intelligence? (Online). Stanford University. [Pub 2007 Nov 12; Cited 2023 Apr 24]. Available online from https://www-formal.stanford.edu/jmc/whatisai.pdf
2. World Health Organization. Rapid Review of WHO COVID-19 Surveillance: External Review. 2021. Available online: https://www.who.int/publications/m/item/rapid-review-of-who-covid-19-surveillance-external-review-27-october-2021
3. Ghosh N, Saha I, Sarkar JP, Maulik U. Strategies for COVID-19 Epidemiological Surveillance in India: Overall Policies Till June 2021. Front Public Health. 2021; 9: 708224
4. Baker, M.G.; Forsyth, A.M. The new International Health Regulations: A revolutionary change in global health security. N. Z. Med. J. 2007, 120, 1267
5. Chen F., Neill D.B. Non-parametric scan statistics for event detection and forecasting in heterogeneous social media graphs. In: Proceedings of the 20th ACM SIGKDD conference on knowledge discovery and data mining, 2014. p. 1166–1175
6. Chae S., Kwon S., Lee D. Predicting infectious disease using deep learning and big data. Int J Env Res Public Health. 2018;15(8) doi: 10.3390/ijerph15081596
7. Basuroy T. Internet penetration rate in India 2007-2022. Statista [Online]. Available online from https://www.statista.com/statistics/792074/india-internet-penetration-rate/
8. Anon. Epidemic Intelligence. Pan American Health Organization. Available online from https://www.paho.org/en/topics/epidemic-intelligence
9. Borda, A.; Molnar, A.; Neesham, C.; Kostkova, P. Ethical Issues in AI-Enabled Disease Surveillance: Perspectives from Global Health. Appl. Sci. 2022, 12, 3890. https://doi.org/10.3390/app12083890
10. Sathish Kumar L, Routray S, Prabu AV et al. Artificial intelligence based health indicator extraction and disease symptoms identification using medical hypothesis models. Cluster Comput (2022). https://doi.org/10.1007/s10586-022-03697-x
11. Kostkova, P.; Szomszor, M.; St. Louis, C. #swineflu: The use of twitter as an early warning and risk communication tool in the 2009 swine flu pandemic. ACM Trans. Manag. Inf. Syst. 2014, 5, 1–25
12. Kostkova P, Mano V, Larson HJ et al. VAC Medi+board: Analysing Vaccine Rumours in News and Social Media. DH '16: Proceedings of the 6th International Conference on Digital Health Conference April 2016 Pages 163–164
13. Epidemic Intelligence from Open Sources: Zero Impact from Health Threats. World Health Organization. Geneva. Available online from https://www.who.int/initiatives/eios
14. Shahid N, Rappon T, Berta W. Applications of artificial neural networks in health care organizational decision-making: A scoping review. PLoS One. 2019; 14(2): e0212356
15. Flood D, Seiglie JA, Dunn M et al. The state of diabetes treatment coverage in 55 low-income and middle-income countries: a cross-sectional study of nationally representative, individual-level data in 680 102 adults. The Lancet Healthy Longevity 2021; 2: E340-51
16. Goss EP, Vozikis GS. Improving Health Care Organizational Management Through Neural Network Learning. Health Care Management Science. 2002;5(3):221–7
17. Bellemo V, Lim ZW, Lim G et al. Artificial intelligence using deep learning to screen for referable and vision-threatening diabetic retinopathy in Africa: a clinical validation study. The Lancet Digital Health 2019; 1: E35-44
18. Abràmoff MD, Lavin PT, Birch M, Shah N, Folk JC. Pivotal trial of an autonomous AI-based diagnostic system for detection of diabetic retinopathy in primary care offices. NPJ Digit Med. 2018;1:39
19. Vial A, Stirling D, Field M, Ros M, Ritz C, Carolan M, Holloway L, Miller AA. The role of deep learning and radiomic feature extraction in cancer-specific predictive modelling: a review. Transl Cancer Res 2018;7(3):803-816. doi: 10.21037/tcr.2018.05.02
20. Vallières M, Freeman CR, Skamene SR, et al. A radiomics model from joint FDG-PET and MRI texture features for the prediction of lung metastases in soft-tissue sarcomas of the extremities. Phys Med Biol 2015; 60: 5471
21. Parag P, Hardcastle TC. Shortage of Radiologists in Low to Middle Income Countries in the Interpretation of CT scans in Trauma. Bangladesh Journal of Medical Science 2022; 21: 489-91
22. Arora R. The training and practice of radiology in India: current trends. Quant Imaging Med Surg. 2014; 4(6): 449–450
23. Nimri R, Battelino T, Laffel LM, et al. Insulin dose optimization using an automated artificial intelligence-based decision support system in youths with type 1 diabetes. Nat Med. 2020;26:1380–1384
24. Nomura A, Noguchi M, Kometani M et al. Artificial Intelligence in Current Diabetes Management and Prediction. Curr Diab Rep. 2021; 21(12): 61
25. Alabdaljabar MS, Hasan B, Noseworthy PA et al. Machine Learning in Cardiology: A Potential Real-World Solution in Low- and Middle-Income Countries. J Multidiscip Healthc. 2023; 16: 285–295
26. Bhavnani SP, Sola S, Adams D, Venkateshvaran A, Dash PK, Sengupta PP. A randomized trial of pocket-echocardiography integrated mobile health device assessments in modern structural heart disease clinics. JACC Cardiovasc Imaging. 2018;11(4):546–557
27. Filho LA, Randhawa VK, Maciel AT et al. We need to talk about critical care in Brazil. Clinics (Sao Paulo). 2022 Jan-Dec; 77: 100096
28. Hunter OF, Perry F, Salehi M et al. Science fiction or clinical reality: a review of the applications of artificial intelligence along the continuum of trauma care. World Journal of Emergency Surgery 2023;18: Article number: 16
29. Nagpal S, Pal R, Ashima, Tyagi A, Tripathi S, Nagori A, Ahmad S, Mishra H.P., Malhotra R, Kutum R, et al. Genomic Surveillance of COVID-19 Variants With Language Models and Machine Learning. Front. Genet. 2022;13:858252
30. Paul D, Sanap G, Shenoy S, Kalyane D, Kalia K, Tekade RK. Artificial intelligence in drug discovery and development. Drug Discov. Today. 2021;26:80–93
31. Álvarez-Machancoses Ó, Fernández-Martínez JL. Using artificial intelligence methods to speed up drug discovery. Expert Opin. Drug Discovery. 2019;14:769–77
32. Venkatesh KP, Raza MM, Kvedar JC. Health digital twins as tools for precision medicine: Considerations for computation, implementation, and regulation. npj Digital Medicine 2022; 5: Article number: 150
33. El Azzaoui A, Kim TW, Loia V, Park JH. Blockchain-based secure digital twin framework for smart healthy city. [Accessed on 26 Apr 2023]. Adv. Multimed. Ubiquitous Eng. 2021; 716: 107–13
34. ReportLinker. Global Digital Twin Market, By Type, By Technology, By Application, By End User, By Region, Competition, Forecast Opportunities, 2017–2027F. Available online: https://www.reportlinker.com/p05778901/Global-Digital-Twin-MarketByApplication-By-End-User-Sector-By-Region-Competition-Forecast-Opportunities.html
35. Mo X, Zhang L, Li H, Qu Z. A novel air quality early-warning system based on artificial intelligence. Int. J. Environ. Res.Public Health 2019; 16: 3505
36. Air quality and pollution city ranking. IQAir [Online]. [Updated 2023 Apr 26]. Available online from https://www.iqair.com/in-en/world-air-quality-ranking
37. Bellinger C, Jabbar MSM, Zaïane O, Osornio-Vargas A. A systematic review of data mining and machine learning for air pollution epidemiology. BMC Public Health. (2017) 17:907. 10.1186/s12889-017-4914-3
38. Ubah JI, Orakwe LC, Ogbu KN et al. Forecasting water quality parameters using artificial neural network for irrigation purposes. Scientific Reports 2021; 11: Article number: 24438

Dr Rudrajit Paul is a consultant Physician at Ruby General Hospital, Kolkata. A former medical professor and HIV master trainer of NACO, he is keenly interested in clinical research and has published numerous articles in indexed international journals. His research interests include climate change and human health, infectious diseases etc.

Dr Meera Suresh is an Associate Professor in the Department of Homeopathy at Lincoln University College, Malaysia. She was also the Program Manager of KDPP-WDF project at SCTIMST which was aimed to reduce Diabetes incidence in Kerala. She is a Homeopathic physician with interest in public health research.

