Turning Healthcare Data into Action: How Guideline-Driven AI Enables Actionable Clinical Workflows
Dr. Martin J. McKeown, Professor and Head of the Division of Neurology, University of British Columbia and the John Nichol Chair in Parkinson's Research
Dr. Z. Jane Wang, Professor, Department of Electrical and Computer Engineering, University of British Columbia
Most healthcare AI focuses on diagnosis or data aggregation. Yet without context aligned to clinical guidelines, extra information just increases cognitive burden without necessarily improving care. Here we argue for agentic, guideline-driven AI that embeds clinical logic to support clinical decision-making.
The Paradox at the Heart of Healthcare AI
Artificial intelligence (AI) has made impressive advances in healthcare, particularly in areas such as image-based diagnosis, note-taking, risk prediction, and data integration. But its impact on everyday clinical care has been surprisingly modest. The reason is a misalignment between what these systems are designed to do and what clinicians actually need.
Most current AI approaches tacitly assume that better diagnosis or more comprehensive data will automatically lead to better clinical decisions. They rarely do. Clinicians are constrained by time, attention, and the difficulty of interpreting information in context. The result is that most current systems generate more alerts, more predictions, and more dashboards, while leaving physicians to figure out what any of it means for patient management. This is not a failure of AI capability but rather a failure of purpose: most efforts have been optimised to generate information, while the real bottleneck is translating it into action.
Why the Field Got Here
Healthcare AI has been largely shaped by computer scientists working with benchmark datasets rather than in real, dynamic clinical environments. This created a natural bias toward problems that are technically tractable (e.g., classification, prediction) rather than those that are clinically meaningful.
But clinical care is fundamentally a dynamic management problem, not a simple classification or prediction problem. Physicians are not simply identifying conditions; they are continuously weighing the pros and cons of potential interventions (including considering no intervention at all), often under uncertain circumstances. Even a highly accurate AI prediction model that does not clearly fit into a decision pathway or change management is not clinically meaningful.
What is missing from most existing AI systems is an explicit representation of clinical reasoning and judgment. Detecting that a patient may be experiencing depression, for instance, is only part of the problem. The harder question is whether this finding should trigger a change in management, and if so, what change. Most systems stop at detection, leaving this critical step entirely to the clinician.
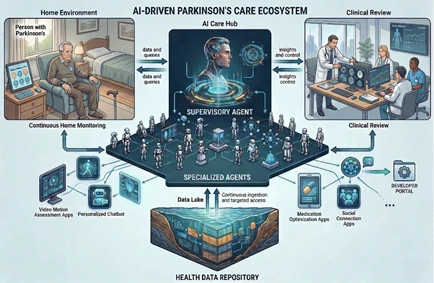
Figure: A multi-agentic AI approach to healthcare. A supervisory agent serves as the primary contact for the person with Parkinson’s disease that can communicate directly with the medical team. The agents continuously scan the Data Lake for actionable events.
Why this matters for healthcare leaders
Chronic conditions such as Parkinson’s disease often lead to predictable, preventable complications, such as depression, hallucinations, and motor deterioration. Proactive early detection and outpatient interventions can significantly reduce unnecessary emergency visits and hospitalisations. In the acute setting, these patients frequently face medication delays, unfamiliar environments, and rapid decompensation, often resulting in prolonged stays, more complications, and substantially higher costs. Prioritising early outpatient management enables health systems to achieve meaningful cost savings by avoiding expensive inpatient care while delivering superior quality outcomes, such as lower readmission rates and improved patient and caregiver quality of life.
Agentic AI: From Passive Analysis to Active Interpretation
Agentic AI offers a different approach. Rather than building a single monolithic model, it uses multiple specialised components (Agents). Each agent is responsible for a specific clinical condition or disease complication, such as mood, sleep, mobility, and medication side These agents evaluate patient-generated data continuously, not just to detect abnormalities, but to assess whether those abnormalities are clinically meaningful and warrant action.
The unifying principle is that all data are interpreted through the lens of care management. The question shifts from “what does the data show?” to “does this information suggest a need to change care?”
Central to this is the explicit encoding of clinical guidelines within the system itself. Guidelines provide evidence-based recommendations for managing specific conditions and complications. By embedding them into agentic AI systems, patient data can be continuously evaluated against established standards of care: Does a change in symptoms meet validated thresholds for intervention? How urgent is the finding relative to other active issues?
It is precisely this action-oriented perspective that transforms a large “Data Lake” into a true decision-support environment. The Data Lake integrates all clinically relevant information for disease management, including demographics, medical history, clinical assessments, medication use, and longitudinal changes in symptoms and treatment response. This approach focuses on actionable findings and aligns the system with how clinicians actually think and work. Unlike traditional alert systems or predictive models, it prioritises actionable decisions rather than simply generating more information.
Human-in-the-Loop: Augmentation, Not Replacement
The system repackages clinical information, applies clinical guideline-based reasoning, and presents structured, interpretable recommendations to the clinician, who then evaluates those recommendations in context and decides what to do.
This approach preserves accountability and clinical oversight while reducing the cognitive burden of information processing. Recommendations can be traced back to specific data inputs and guideline logic, making the system transparent rather than opaque. The physician is not a rubber stamp but rather the primary decision-maker the system is built to support.
Toward Continuous, Proactive Care
Most healthcare is still organised around episodic clinic visits. Between visits, patients may develop complications that go unrecognised until they become severe enough to prompt urgent care.
Agentic, guideline-driven systems support continuous monitoring. By evaluating patient data in real time, they can flag emerging issues early and prompt timely intervention, potentially reducing avoidable crises and making more efficient use of clinical resources. For chronic disease management, especially where ongoing adjustment of care matters more than a single point diagnosis, this is a significant shift.
For healthcare systems, the practical implications include replacing unstructured triage (phone calls, ad hoc messages) with structured, prioritised information and ensuring that clinician attention is directed toward the most clinically relevant issues.
Importantly, these benefits depend not only on the technology itself, but on its integration into existing care pathways. In contrast, systems that are not aligned with standard clinical workflows are unlikely to succeed, regardless of their technical sophistication.
For example, in a Parkinson’s remote monitoring system, patient data from chatbots, wearables, and video-based assessments can be continuously evaluated by specialised agents against clinical guidelines. When a meaningful change is detected, such as worsening depression meeting intervention thresholds, the system generates a prioritised, guideline-based alert. Clinicians receive a structured summary of the issue, its urgency, and recommended management pathways, enabling timely intervention (e.g., medication adjustment or referral) while preserving clinical oversight.
What Needs to Change
Realising this vision will require changes in how healthcare AI is designed, developed and deployed. Closer collaboration between clinicians and engineers is essential, not only at the level of data sharing and analysis, but in defining the problems to be solved and the criteria for success.
Design goals must shift from AI models maximising predictive performance to enabling meaningful clinical action. This includes embedding guideline-based reasoning, ensuring interpretability, and integrating outputs into workflows in ways that support, rather than disrupt, care delivery.
Regulatory Considerations and Validation
Deploying agentic, guideline-driven AI in clinical settings requires alignment with applicable regulatory frameworks governing medical software. By explicitly grounding outputs in government-published clinical guidelines and ensuring the system presents structured information rather than autonomous treatment recommendations, developers can more clearly define the software's boundaries.
Rigorous validation remains essential to demonstrate that guideline logic is accurately implemented, outputs are clinically appropriate across relevant patient populations, and workflow integration does not introduce new sources of error. Such a structured, guideline-based approach is more likely to comply with regulatory constraints than many current opaque, model-driven systems. Addressing these requirements early in development, rather than retroactively, is central to responsible deployment.
Limitations and Potential Pitfalls
Despite the potential of such an Agentic, guideline-driven AI approach, several challenges remain. First, the system's value depends entirely on the quality of patient-generated data. Guideline-based reasoning applied to unreliable data does not produce cautious recommendations, but rather confidently wrong ones. Robust data quality monitoring is therefore essential.
Second, clinical guidelines often reflect the populations from which evidence was gathered, and some populations may be underrepresented in training data. Embedding guidelines into an automated system risks scaling existing disparities rather than correcting them. Developers must actively audit guideline logic for equity implications, particularly when deploying across diverse patient populations.
Third, the human-in-the-loop model, while conceptually sound, can degrade in practice. When clinicians receive a continuous stream of structured recommendations, habituation sets in. Outputs that are technically reviewable become automatically approved. This is a subtler form of the “alert fatigue problem” seen in current systems.
Conclusion
Healthcare AI currently excels at perception and prediction, but not yet at helping clinicians to act more quickly, consistently, and with greater confidence. The shift we are arguing for is not a rejection of what came before. Accurate diagnosis and data integration remain vital, but they should be intermediate goals rather than final outcomes of healthcare AI systems. A system that flags a risk without guiding the response has done only half the job. This system can be incrementally deployed by including guideline-driven agents into existing patient monitoring and EHR systems.
Agentic, guideline-driven AI represents a more complete vision: one in which clinical knowledge is embedded in the system itself, findings are filtered through the lens of management, and the clinician receives not just information but a reasoned basis for action. The human remains in the loop not as a fail-safe, but as the decision-maker the system is designed to support. We suggest that the future will depend not just on garnering more data, but on smarter approaches to turning data into actionable decisions, and we now have the tools to build it.

Dr. Martin J. McKeown is a Professor and Head of the Division of Neurology at the University of British Columbia and the John Nichol Chair in Parkinson’s Research. Trained in both engineering and medicine, his work focuses on AI-driven approaches to neurological disorders, including digital biomarkers and clinical decision support systems. He leads interdisciplinary research integrating neuroscience, engineering, and machine learning to improve patient care and clinical workflows.

Dr. Z. Jane Wang is a Professor in the Department of Electrical and Computer Engineering at the University of British Columbia. An IEEE Fellow and Fellow of the Canadian Academy of Engineering, her research focuses on signal processing, machine learning, and biomedical data analytics. She has authored over 200 journal publications and leads interdisciplinary work applying AI to complex biomedical and digital health challenges.

