The Financial Toll of In-Patient Falls: A Study on Costs and Prevention
Yogamaya Nayak, Healthcare Quality Assurance Expert
Gaurav Loria, Senior Healthcare Executive
Seerat Thind, Dentist, IIHMR University
Nishant Nishit, Healthcare Professional
The purpose of this research study is to examine the consequences of falls that occur while patients are admitted to the hospital. It emphasizes the importance of implementing strategies to prevent incidents. The study was conducted retrospectively examining fall data from January to June 2023 in more than 40 multi-speciality hospitals. The data sources used included incident reports from hospitals and medical records. This study provides an understanding of how falls impact healthcare by considering immediate medical costs and prolonged hospital stays. It underlines the need for targeted prevention measures that can effectively reduce fall incidents and their associated expenses. Healthcare professionals and policymakers can utilize this study as a resource when developing strategies, for fall prevention.

In-patient falls pose a significant risk to patient safety and impose a substantial financial burden on healthcare institutions. By comprehensively analyzing the direct and indirect costs associated with patient falls, this research aims to shed light on the economic impact and inform healthcare providers and policymakers about the urgency of implementing effective fall prevention strategies.
Objective
This study aims to identify and evaluate the cost implications of in-patient falls in hospitals.
Design, Setting & Methodology
A retrospective observational study was conducted at more than 40 multi-speciality hospitals. Patients with a history of falls in the hospitals were considered from 1st January to 30th Jun 2023. In-patient falls data was collected from hospital online incident reporting data base and medical record reviews. A primary data collection method was employed, using datasets already available for patient medical records. The medical records of in-patients were studied to find out the cause, consequence, and management of patients. Patient bills were linked to the falls to calculate the cost of each fall.
Results
A total of 246 in-patient falls occurred during the specified period. Our study indicates that the in-patient fall rate among patients of the vulnerable category was higher. Among the patients who had a fall, 59% had to undergo at least one radiological investigation such as NCCT head, an x-ray of arm, foot, shoulder, pelvis, etc., amongst which 31% of investigations done were NCCT head. Results from this study have provided a comprehensive understanding of the financial impact of in-patient falls, including the immediate medical costs and the cost of extended hospital stays.
INTRODUCTION
According to the World Health Organisation, a fall is an event that results in a person coming to rest inadvertently on the ground, floor, or other lower levels. Such falls may become deadly for several individuals, such as the elderly, physically disabled, mentally challenged, etc.
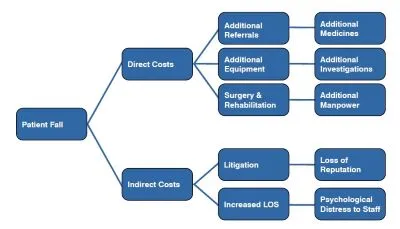
Consequences of a fall include both direct and indirect costs. Direct costs include increased length of stay, medicines, investigations such as an x-ray, CT, etc., while the indirect costs include transportation and lodging of patient’s attendants, absence from work resulting in loss of wages, cost of food services, prolonged fear of fall, mental distress, etc.
The financial impact of fall-related injuries is substantial, however, there is insufficient research on the costs of patient falls in healthcare systems.
DATA ANALYSIS
Incidence of falls
Our study included 246 unique patients and a total of 3,59,344 patient hospital admissions over a period of January to Jun 2023.
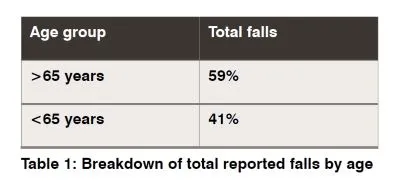
1. Incidence of falls by age and gender
In our study, it was observed that 65 years and older patients suffered more falls. 85.7% of these patients had pre-existing co-morbidities such as hypertension or diabetes mellitus.
• The study indicates that there is higher occurrence of falls among male patients. This observation may be attributed to a higher number of hospital admissions for males.
• The data reveals that 89% of men who fell had underlying health issues that may cause weakness, impaired balance and an increased likelihood of falling.
• Around 76% of all male patients who experienced falls were prescribed medications known to have a high risk of causing falls, such as antihypertensives, benzodiazepines, antidepressants, etc.
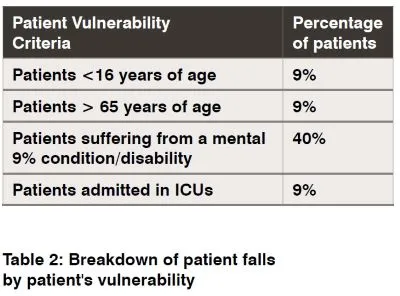
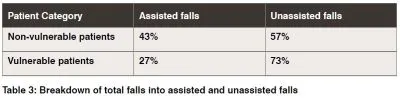
2. Incidence of falls by the vulnerability of patients
Vulnerable patients are the ones who are:
• Chronically ill or disabled
• Patients <16 years and >65 years
• Patients admitted in ICUs
• Patients suffering from a mental condition/disability
67% of all patients with a history of falls were vulnerable (because of old age, weak limbs and muscles, underlying comorbidities, heavy doses of medications, reduced immunity, chronic disabilities, etc.), hence, at a higher risk of falls.
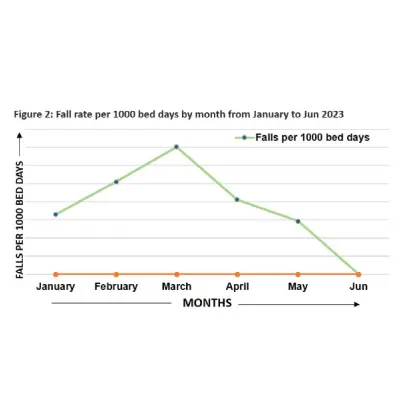
3. Incidence of falls per 1000 bed days
The average number of admissions per month was reported to be ~59890, while the average occupied bed days were ~9678 from January to Jun 2023.
From this data, we calculated the monthly fall rates per 1000 bed days.
Falls per 1000 bed days = (Number of falls * 1000) / occupied bed days
• The fall rate per 1000 bed days is the highest in March because of higher number of hospital admissions, and lowest for January.
• The average length of stay (LOS) for the period was 3.92.
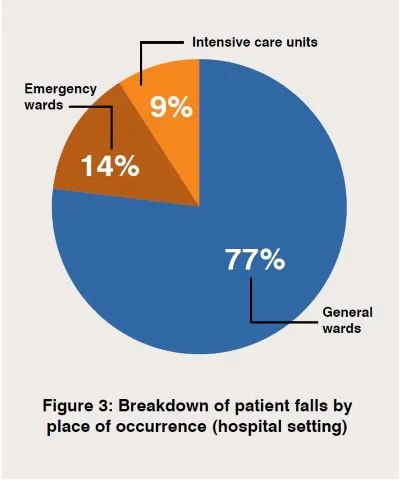
4. Incidence of falls based on the place of occurrence (hospital setting)
At least 77% of patient falls took place in the general wards. Other hospital areas include the emergency wards and intensive care units.
• This study found that the maximum falls occurred in the general wards because 64.7% of patients admitted to these wards were unassisted.
• Irrespective of fall prevention measures being followed, 78% of falls occurred when the patient did not ring the call bell to ask for assistance.
• Amongst those unassisted patients, 63% of falls occurred inside the washroom, while the rest occurred when the patient tried to move out of bed or perform an activity on the bed.
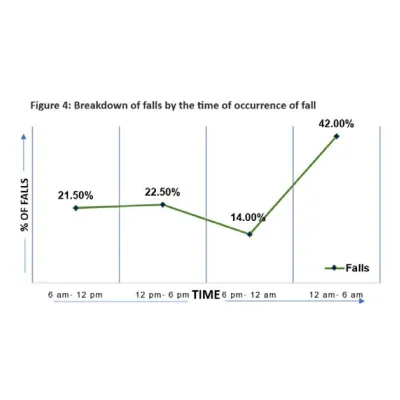
5. Incidence of falls based on time of occurrence of falls
The study indicated that most numbers of falls occurred during 12 - 6 am, i.e., approximately 42%.
• It was interpreted that falls during this period occurred because 68% of patients were unassisted at the time of fall.
• The reason could be the patient’s unwillingness to request assistance at night or early morning hours.
• Before bedtime, most patients were given medicines such as sedatives, benzodiazepines, anti-hypertensives, etc. These drugs may cause sleepiness and dizziness and can lead to falls.
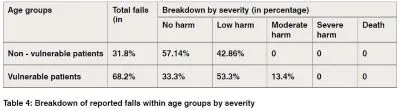
6. Incidence of falls based on the severity of harm caused
A report by the National Patient Safety Agency (NPSA) in 2007 applied falls definitions to these categories:
a) No harm: where no harm came to the patient, e.g., no visible bruising.
b) Low harm: required first aid, minor treatment, or medication, e.g., graze on the right hand.
c) Moderate harm: likely to require outpatient treatment, surgery, or a longer stay in the hospital, e.g., fractured pubic rami.
d) Severe harm: where permanent harm, such as brain damage or disability occurred e.g., fractured neck of femur.
e) Death: where fall resulted in death.
• As per falls by severity, 68.2% of total falls occurred among vulnerable patients.
• The vulnerable patients are more likely to suffer moderate to severe harm, as these patients are weaker, and more susceptible to harm.
• Rehabilitation services mainly included physiotherapy.
• The surgery done for patients with a history of falls was to treat fractures of arms and legs.
• The maximum number of services, including surgery and rehabilitation were provided to the vulnerable patients.
• For further management of falls, patients were referred to specialists in neurosurgery, general surgery, and orthopedics.
• Additional referrals and investigations for fall account for the highest number of services provided.
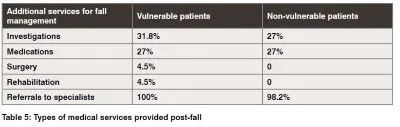
7. Additional medical costs by services
Our study indicated that among all the clinical services provided to fall patients, imaging services and referral to specialists were the most used services, followed by medical services.
• Imaging services were used in 59%, while medication services were used in 50% of all cases.
• NCCT or Non-Contrast Computed Tomography head/brain was the most used imaging service. 30.7% of all investigations done were NCCT head, followed by X-ray pelvis which was 19.2% of all investigations. Other post-fall investigations included an X-ray of the spine, arm, foot, knee, shoulder, MRI, etc.
• Each patient was referred to at least 3 specialties for the management of falls, i.e., surgery, neurosurgery, and orthopedics. The maximum number of referrals given was 6, while the mean or average was 5 referrals.
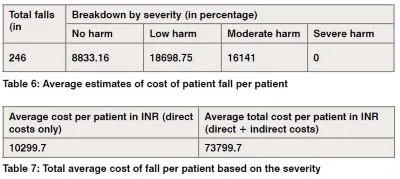
8. Estimation of the average total cost of fall
On the estimation of the average cost of fall per patient, these assumptions were made
a. Each patient who suffered a fall, stayed in the facility for one additional day (additional LOS).
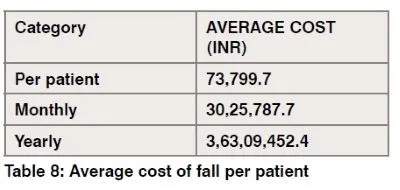
b. The average number of monthly falls that occur was assumed to be 41. Around INR 74,000 is spent on managing one fall over six months from January to Jun 2023.
• It was further interpreted that indirect costs such as additional LOS constitute the major part of expenditure as indirect costs account for 7 times the direct costs in the total expenditure.
• On the further breakdown of cost analysis per patient per fall, we found that patient falls that resulted in low harm incurred the maximum expenditure on the management of a single fall.
• Furthermore, the monthly expenditure on the management of falls is approximately INR 30,25,787.
• Thus, in a year the facility spends approximately INR 3,63,09,452 on the management of falls.
DISCUSSION
In a healthcare facility, patients are regularly monitored for risk of falling. A fall risk assessment tool is used to assist in the same. The fall risk assessment tool consists of a scoring system on the patient’s details, such as vulnerability criteria, clinical history, diagnosis, mental health condition, prescribed medications, etc. All these criteria are given a score and the total score is calculated. If the score is equal to or greater than 45, the patient is at a higher risk of falls, and thus needs to be monitored intensively.
Patients and their family members/attendants are also given periodic education on fall prevention measures. These measures include the usage of a call bell for assistance, keeping bedside rails raised, instructions given on– raising, sitting, and moving out of the bed, etc. Additional measures taken by the hospital staff include placing a ‘safety first’ sticker, a fall risk band application, assisting with toilet needs, frequent visits to check the patient, etc.
Stringent measures are being followed along with patient-family education to prevent falls however, patient falls still pose a risk. The environment or methodology of implementing fall prevention measures may not give desired results for which there are several possible reasons. Firstly, the method of education is standard for all, thus it does not communicate to each patient individually. Secondly, it is generalized for all categories of patients, irrespective of the patient’s vulnerability to falls. Lastly, these measures are communicated without understanding if the patient is receptive to these measures because of the patient’s condition or literacy, or cognition. More robust preventive measures to strengthen patient education in such a way that it brings out the desired results is the need of the hour.
The potential savings from reducing falls in hospitals are also substantial. Over the course of a year, the facility spent around INR 3,63,09,452 on fall-related expenses. Strategically reinvesting the savings generated from reducing patient falls can greatly improve healthcare technologies that aim to prevent falls. One such technological advancement involves using sensor-based alarms and remote monitoring systems. These innovative solutions utilize sensors and smart devices to detect movements and instantly alert nurses and attendants enabling them to respond quickly and prevent falls. Additionally implementing these cutting-edge solutions can result in long-term cost savings by reducing fall-related injuries minimizing hospital stays and improving efficiency in care.
References:
Cascella, L. M. (n.d.). 15 ways hospitals can improve environmental safety and reduce falls.
Commission, T. J. (2015, September 28). Preventing falls and fall-related injuries in health care facilities. Sentinel Event Alert.
David Meddings, R. (n.d.). step safely: strategies for preventing and managinf falls across the life course . WHO.
Ethan U. Cumbler, J. R. (2013). Inpatient falls . PubMed Central.
Hazel Heng, D. J. (2020). Hospital falls prevention with patient education: a scoping review. BMC Geriatrics.
Hirose, M. (2018). additional medical cost of hospital acuired falls . journal of patient safety .
Hirose, M. (2018). additional medical costs due to hospital acquired falls . journal of patient safety .
Hirose, M. (2018). additonal medical costs due to hospital-aquired falls . journal of patient safety .
Hirose, M. (n.d.). additonal medical costs due to hospital acquired falls . journal of patient safety .
how much do patients fall cost in your facility. (n.d.). AliMed.
Jennifer R Simpson, L. D. (2013). Inpatient Falls: Defining the Problem and Identifying Possible Solutions. Part II. PubMed Central.
Lee Adler, D. Y. (2018). Impact of Inpatient Harms on Hospital Finances and Patient Clinical Outcomes. Journal of Patient Safety.
Masahiro, H. (2018). additional medical costs of hospital-acquired falls. journal of patient safety .
Masahiro, H. (n.d.). additional medical costs due to hospital-acquired falls . journal of patient safety .
Patricia C Dykes, M. C.-B. (2023). Cost of Inpatient Falls and Cost-Benefit Analysis of Implementation of an Evidence-Based Fall Prevention Program. PubMed Central.
(oct 2016). Preventing Patient Falls: A Systematic Approach from the Joint Commisiion Centre for transforming healthcare project. Chicago: Health Research & Educational Trust.
(2016). Preventing Patient Falls: A Systemic approach from The joint Commission Centre for transforming healthcare project. Health Research & Educational Trust.
Raju Vaishya, A. V. (2020). Falls in Older Adults are Serious. PubMed Central.
Rob Moriis, s. o. (2017). Prevention of falls in hospital. royal college of physicians .
Rob Morris, S. O. (2017). prevention of falls in hospital. PubMed Central.
Rob Morris, S. O. (2017). Prevention of falls in hospital. PubMed Central.
Warren, C. (2023). A comprehensive analysis of risk factors associated with inpatient falls. journal of patient safety.
(n.d.). WHO GLOBAL PATIENT SAFETY ACTION PLAN 2021–2030 Towards eliminating avoidable harm in health care. WHO.
Author Bio

Yogamaya Nayak is a Six Sigma Green Belt certified healthcare quality assurance expert, dedicated to improving patient experience and safety measures. With a proven track record of coordinating, auditing, and solving problems in various hospital settings, she is committed to ensuring compliance and excellence in healthcare delivery.

Gaurav Loria is a senior healthcare executive with over 16 years of experience in leading and transforming hospitals, clinics, and healthcare IT. He's a visionary leader who is committed to uplifting global healthcare standards and prioritizing patient safety.

Dr Seerat Kaur, a dedicated dentist, is on a transformative journey. Her passion for patient care led her to pursue an MBA in Health and Hospital Management at IIHMR University, Jaipur. Balancing dentistry with healthcare leadership, Dr Seerat aims to leave a lasting impact on the industry, bridging care and management.

Nishant Nishit is a healthcare professional and an author. He uses his expertise to educate and empower patients and healthcare providers. He is passionate about improving patient safety, quality of care, and health outcomes through evidence-based practices and communication.

