Postoperative Pain Management, Esp. Thoracic Surgery
Paul Swatek, OA for thoracic surgery, Medical University of Graz
Postoperative pain is one of the biggest problems in surgery, esp. in thoracic surgery. There are currently many guidelines for postoperative management available, such as the one of the American pain society. These guidelines provide a good standard, but they cannot reflect the individual situations in every surgical procedure and therefore sometimes they have to be adopted especially for the individual person. Besides medication, local anesthesia and line block, minimal invasive surgery and robotic assisted surgery is performed to achieve better pain management.

Choosing the correct setting in pain management suitable to the patient is key to rapid recovery after surgery. Postoperative pain in surgery, especially in thoracic surgery, is one of the main reasons for
Immobility and therefore postoperative complications such as pneumonia or prolonged hospitalization. There are several guidelines available, such as the American pain society or the American society of anesthesiologists. They suggest a wide arrange of drugs and procedures such as regional nerve blocks to manage the pain in postoperative patients.
After surgery, up to 75% of the patients suffer from acute postoperative pain of a medium to high intensity. More than 50% of those patients report an inadequate pain relief in the treatment of the pain. These patients are at risk of developing a chronical pain syndrome associated with surgery. Up to 10% of the patients undergoing surgery suffer from severe persistent postoperative pain, which is verry difficult to treat.
Anatomy and Physiology
There are afferent nerves that mediate the pain sensation towards the central nervous system. Postoperative pain can be categorized as nociceptive, inflammatory, or neuropathic pain, all meditated by a different kind of neural pathways. Neuropathic pain is getting mediated by activated unmyelinated C-fibers, thinly myelinated A-delta-fibers, and myelinated A-beta-fibers. It occurs as a result of a noxious stimuli such as tissue damage performed for example by the incision of the skin during the operation. Inflammatory pain occurs when nociceptive nerval fibers get sensitized in the response to the release of inflammatory mediators such as cytokines. This is usually associated with the clinical signs of inflammation, as there would be clinical evidence of heat, pain, erythema and swelling in or near the operation field. The pain sensation can last from several hours to days and usually improves when the inflammation is gone. Usually, there will be no persisting pain as a result of an inflammation. Neuropathic pain is the result of an injury of the nerval structure, which leads to an increased axonal sensitivity to stimuli of the peripheral nerve. This kind of pain will manifest shortly after surgery and has the potential to persist as chronic postoperative pain over several months and in worst case even longer.
In addition to the categorization above postoperative pain is also characterized as somatic or visceral. Somatic pain is the input of nociceptive myelinated, rapidly conducting fibers found in cutaneous and deep tissue, which contribute to a more localized, sharp quality of pain. The category of visceral pain is conducted over a neuronal network of fibers that spreads across multiple viscera and combines before entering the spinal cord in the dorsal root. There are also connecting fibers towards the autonomous nerval system. This is why the visceral pain is not only more diffuse and not clearly localizable pain, but also it can also be accompanied by autonomic reactions such as alternating blood pressure or influencing the heart rate of the patient.
The aim of different therapeutic intervention is to target these afferent structures in various ways. Antagonizing pain receptor activity, blocking the production of pro-inflammatory mediators or simply blocking the afferent nerve are only a few ways to improve postoperative pain management.
Measuring the pain
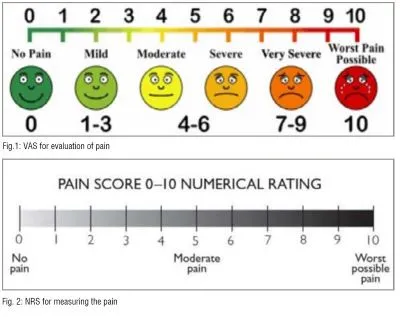
In general, it is verry difficult to measure pain, because there are nearly none objective measurements available. There are several individual factors that can influence the pain in patients, such as age, gender, social background, etc. In the time of migration there are sometimes a lot of problems in communicating with the patients, making it difficult for patients and the medical stuff to evaluate the pain. There are several scales available for quantizing pain, many of those require communication. Widely used therefore is the Visual Analog Scales (VAS) and the numerical rating scales (NRS).
Systematic overview
In 2012 the American Society of Anesthesiologists (ASA) published a guideline for acute postoperative pain management, which was approved by the American Society of Regional Anesthesia and Pain Medicine. There are several pre-, inter- and postsurgical interventions and management strategies are available to reduce the postoperative pain of the patients.
Systemic pharmacologic therapy
The systemic application of opioids, NSAID (non-steroidal anti-inflammatory drugs), acetaminophen, gabapentin, ketamine or lidocaine or many other substances is widely used in pain management. Oral application of opioids is preferable to the intravenous route. Nevertheless, there are situations, where oral medication is not the way to go. Extreme pain or non-ability to digest the medication during an Ileus or other circumstances could lead to the fact, that oral medication cannot be applied. In that case, the intravenous route has to be chosen and therefore the ASA recommends the form of patient-controlled anesthesia in those patients.
Local, Intra-articular, or topical techniques
That kind of site-specific pain control is not in wide use. They could be considered individually but there is no general recommendation for these procedures.
Regional anesthetic techniques
A local anesthetic with or without the addition of IV opioid medication is an option for fascial plane block, site-specific regional anesthetic injections, or in some cases epidural injections depending on the type of procedure performed. These procedures are usually performed under ultrasound guidance. The use of continuous medication IV for general pain control is preferable to singleinjection techniques in cases where the duration of postoperative pain is prolonged. Intrapleural analgesia is not recommended for pain control as there is little evidence to suggest benefit, and high systemic absorption within the pleural space increases the risk of drug toxicity.
Neuraxial anesthetic techniques
The Injection of local anesthetics into the epidural space is often performed in modern surgery. The addition of IV opioid is optional. It can be applied through continuous infusion or also as patient controlled anesthesia, dose-limitation is then mandatory. These techniques are widely used in thoracic surgery, extended abdominal procedures as well as Operations on hips and lower extremities. It is also performed in section caesarian, because there is verry little additional necessary and therefore the child is hardly affected.
Nonpharmacologic therapies- ex, cognitive modalities, physical therapy, transcutaneous electrical nerve stimulation (TENS)
In general, additional physiotherapy as well as cognitive modalities are an addition to pharmaceutical or other modalities of pain control. Some of these modalities can start before the operation and is performed in some centers.
Surgical techniques
In recent past not only the anesthesiologic and pharmacological pain management improved, but also the surgical procedures improved a lot when it comes to postoperative pain. The evolution of laparoscopic and thoracoscopic surgery led to less traumatizing procedures because there are less inflammatory mediators released. Therefore, less pain is developed and the pain management is better than in open and conventional surgery. The rise of the robotic surgery in recent years also shows the benefit of less invasive procedures providing and enabling the surgent to perform even more complex resections than by other minimal invasive modalities. With the development of newer robot generations and the broader use of those equipment all over the world the experience within the sergeants will grow and more and more complex operations will be performed by this technique.

Clinical view
There are several factors, that have to be considered when planning the postoperative management of a patient. Besides the factors of the planed procedure there are several individual factors, that have to be considered. These include patient age, history of chronic opioid use, and other comorbidities
Especially obese patients are challenging patients regarding to the use of opioids because they easily develop respiratory deficiency or sleep apnea.
Patients suffering from chronical pain syndrome often require huge amounts of analgesia exceeding their baseline dose. Interventional anesthetic techniques and non-opioid pain management is verry important in these patients.
To be taken into consideration is also the possible misuse of opioids. A pre-existing history of depression or misuse of other substances as well as other risk factors have to be considered when planning on pain management.
Inadequate pain management has severe impact on the patient’s health, including the ability to manage their daily life. Often there are sleeping disorders, reduction of libido, and mood disorders. There is also a higher probability of developing a chronic pain syndrome with initially poor pain management.
The risk in taking opioids show in somnolence, sedation, respiratory depression, urinary retention, nausea/vomiting, ileus, which could lead to death. There is, as already mentioned, the possibility of addiction and substant use disorder and severe withdrawal symptoms when getting of the medication.
There is a bleeding risk in the use of NSAID, which has to be considered in operations, where a big blood loss is to be expected. There is also an increased risk in gastrointestinal bleeding and renal dysfunction.
Peripheral nerval blocks may result in motor blockade of depended muscles, increasing the morbidity and severely reducing the mobilization of the patient.
In neuraxial anesthesia, patients require close monitoring as respiratory depression, hypotension, and motor weakness from spinal cord compression may occur. These are severe complications requiring acute intervention if they occur.
ERAS-Concept
Enhanced recovery after surgery (ERAS) are specially designed multimodal perioperative care pathways with the purpose of earliest possible mobilization and to get the patients back to their daily routine as soon as possible. In the ERAS-Concept, pain management is key to early mobilization of the patient as well as the preoperative preserving of organic function and reducing the stress response after surgical trauma.
Conclusion
Pain management is one of the big tasks to be achieved after surgery, esp. after big resections and thoracic surgery. Less pain in patients lead to a faster recovery and less chance of persisting postoperative pain in the long term. It reduces the days in the hospital and the patient will be able to start his daily routine as early as possible. It is in the best interest of the anesthesiologist, the surgeon and all other participating specialties like the nursing stuff to monitor and manage the pain of postoperative patients to reduce complications in the long run.
References:
1 Hemmerling TM. Pain management in abdominal surgery. Langenbecks Arch Surg. 2018 Nov;403(7):791-803.doi: 10.1007/s00423-018-1705-y. Epub 2018 Oct 3. PMID: 30284029.
2 Schwarzova K, Whitman G, Cha S. Developments in Postoperative Analgesia in Open and Minimally Invasive Thoracic Surgery over the Past Decade. Semin Thorac Cardiovasc Surg. 2023 Sep 30:S1043-0679(23)00104-1. doi: 10.1053/j.semtcvs.2023.07.002. Epub ahead of print. PMID: 37783320.
3 Chou R, Gordon DB, de Leon-Casasola OA, Rosenberg JM, Bickler S, Brennan T, Carter T, Cassidy CL, Chittenden EH, Degenhardt E, Griffith S, Manworren R, McCarberg B, Montgomery R, Murphy J, Perkal MF, Suresh S, Sluka K, Strassels S, Thirlby R, Viscusi E, Walco GA, Warner L, Weisman SJ, Wu CL. Management of Postoperative Pain: A Clinical Practice Guideline From the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists' Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J Pain. 2016 Feb;17(2):131-57. doi: 10.1016/j.jpain.2015.12.008. Erratum in: J Pain. 2016 Apr; 17(4):508-10. Dosage error in article text. PMID: 26827847.
4 Suner ZC, Kalayci D, Sen O, Kaya M, Unver S, Oguz G. Postoperative analgesia after total abdominal hysterectomy: Is the transversus abdominis plane block effective? Niger J Clin Pract. 2019 Apr;22(4):478-484.
5 Lovich-Sapola J, Smith CE, Brandt CP. Postoperative pain control. Surg Clin North Am. 2015 Apr;95(2):301-18.
6 Lespasio MJ, Guarino AJ, Sodhi N, Mont MA. Pain Management Associated with Total Joint Arthroplasty: A Primer. Perm J. 2019;23
7 Maloney J, Wie C, Pew S, Covington S, Maita M, Kozinn R, Sabin M, Freeman J, Kraus M, Strand N. Postthoracotomy Pain Syndrome. Curr Pain Headache Rep. 2022 Sep;26(9):677-681. doi: 10.1007/s11916-02201069-z. Epub 2022 Jul 11. PMID: 35816220.
8 Blichfeldt-Eckhardt MR. From acute to chronic postsurgical pain: the significance of the acute pain response. Dan Med J. 2018 Mar;65(3)
9 Khalil H, Shajrawi A, Dweik G, Zaghmouri A, Henker R. The impact of preoperative pain-related psychological factors on pain intensity post-surgery in Jordan. J Health Psychol. 2021 Dec; 26(14):2876-2885. doi:
10.1177/1359105320937067. Epub 2020 Jun 27. PMID: 32597221.
10 Abu Akar F, Gonzalez-Rivas D, Shaqqura B, Salman W, Ismail M, Safadi T, Adwan R, Al-Hassan H, Rumman N, Hijjeh N. Uniportal video assisted thoracoscopy versus open surgery for pulmonary hydatid disease-a single center experience. J Thorac Dis. 2020 Mar; 12(3):794-802. doi: 10.21037/jtd.2019.12.73. PMID: 32274146; PMCID: PMC7139009.
11 Lespasio MJ, Guarino AJ, Sodhi N, Mont MA. Pain Management Associated with Total Joint Arthroplasty: A Primer. Perm J. 2019; 23
12 Garimella V, Cellini C. Postoperative pain control. Clin Colon Rectal Surg. 2013 Sep;26(3):191-6
13 Gelman D, Gelmanas A, Urbanaitė D, Tamošiūnas R, Sadauskas S, Bilskienė D, Naudžiūnas A, Širvinskas E, Benetis R, Macas A. Role of Multimodal Analgesia in the Evolving Enhanced Recovery after Surgery Pathways. Medicina (Kaunas). 2018 Apr 23; 54(2):20. doi: 10.3390/medicina54020020. PMID: 30344251; PMCID: PMC6037254.
Author Bio

Dr. Paul Swatek did his degree at the medical university of Graz, where he also specialized in thoracic surgery. After several years as a consultant, he took over the department of thoracic surgery at the Klinikum Ingolstadt/Germany. He is specialized in oncological resections and in minimal invasive thoracic surgery with uniportal approach. Today he is working at the medical university of Graz again to examine and develop new approaches on thoracic surgery.

