
Classic Cardiac Devices
Implantable cardiac devices have been part of routine therapy in cardiology for decades. Classic devices have formed a basis for the development of innovative ones. Cardiac pacemakers (PMs) and implantable cardiac defibrillators (ICDs), which are electronic devices usually placed into the chest wall just below the collarbone, and heart valves to be deployed by open chest surgery and later by minimally invasive cardiac surgery (MICS) are such classics.
Pacemakers and Defibrillators
Main indication for PM insertion is to help regulate slow heart rate occurring due to diseases of the electrical conduction system. As a substitute, PMs provide the heart with missing electrical impulses conveyed by electric leads to the right atrium (RA), right ventricle (RV) or both right-sided heart cavities. Percutaneous implantation of an entirely intracardiac leadless PM represents the lates development in this field. No surgery is needed for that kind of PM implantation, which is rather deployed via an endovascular approach from the right femoral vein. However, functionality of leadless PMs is limited to ventricular stimulation. That is why leadless PMs are just suitable for a minority of patients.
In individuals suffering from heart failure due to cardiomyopathies or other extended damage of the heart muscle, timing of electrical stimulation and subsequent response of pumping heart chambers (ventricles) may be altered what often results in asynchrony between left and right ventricular performance and may further worsen heart failure symptoms. Cardiac resynchronization therapy (CRT) has been shown to improve heart failure symptoms in a certain proportion of such patients. Therefore, special PMs with CRT capability are used in patients with asynchrony if positive response is likely.
ICDs are another kind of PM-like devices providing with overdrive pacing or delivering electric shocks if needed. ICD implantation is indicated for primary prevention of sudden death due to ventricular fibrillation or tachycardia (VF/VT) in patients deemed to be on high risk due to poor heart function (severe heart failure) or for secondary prevention if individuals have already survived an event of VF/VT, e.g. after successful resuscitation. PM functionality is inherent to ICDs in order to start pacing once a shock has been delivered. That can also include CRT capability because both, ICD implantation and CRT, may be indicated in the same patient population.
Surgical Valve Replacement
Surgical heart valves belong to the first therapeutic cardiac devices and have been implanted since the sixties. All four cardiac valves can be replaced by open chest or minimal invasive cardiac surgery. Therefore, native heart valves need to be excised to implant artificial ones as a surrogate, durability of which may be limited depending on type and material of those prostheses. An important distinction is made between mechanical and biological ones. The latter are made from cow, pig or human heart tissue. Current mechanical prostheses are characterized by mostly life-long durability but require permanent anticoagulation what entails bleeding risks. Ten to twenty years after implantation, biological valves often have to be replaced again once prosthesis degeneration is progressing. However, they just require short-term anticoagulation followed by long-term therapy with aspirin or another antiplatelet therapy. That is why they are predominantly recommended to be implanted in patients beyond the age of sixty years.
Percutaneous Valve Implantation
In nonsurgical valve replacement, native valves are left in the human body and artificial ones are implanted inside the native valve pushing the latter aside. Consequently, although still in common use, the term nonsurgical or transcatheter “valve replacement” is actually not correct and might be superseded by “valve implantation”.
Percutaneous Aortic Valve Implantation
Transcatheter aortic valve implantation (TAVI) also known as transcatheter aortic valve replacement (TAVR) was the first percutaneous approach for valve therapy when prevalence of calcific aortic stenosis (AS) increased with progressing life-expectancy, since AS is a disease of advanced age. Consequently, an increasing percentage of candidates for surgical aortic valve replacement were deemed on high risk so that TAVI became a therapeutic alternative of utmost importance. Transfemoral access represents the approach of choice and other ones as are transapical, transjugular and transaortic access techniques are just considered surrogates in case the valve prosthesis, which is always a biological one, cannot be advanced through the femoral artery for anatomic reasons, e.g. artery occlusive disease.
Prostheses for TAVI differ according to two deployment techniques as are self-expandable and balloon-expandable ones. The latter are mounted on a balloon and are deployed by inflating the same in a way comparable to coronary stent implantation. Balloon expansion pushes calcific native valve tissue aside which also works as an anker for the TAVI prosthesis. There is no need for sutures what is another difference to surgical valve replacement requiring the prosthesis to be sewed in. In contrast, self-expending prostheses are released from the shaft of a catheter. In some cases, pre-dilatation of the stenotic valve is needed before placing a self-expandible prosthesis. Overall, TAVI has been shown to be safe and feasible. According to recent trials, the use of TAVI extends the scope of high and even intermediate risk surgical candidates and is at the least equivalent to surgical aortic valve replacement. TAVI can also be done after previous biological valve replacement be it surgically or percutaneously. This kind of implantation is called valve-in-valve (ViV) TAVI.
Percutaneous Mitral Valve Implantation
Transcatheter mitral valve implantation or replacement (TMVR) is much less common compared to TAVI. That mitral stenosis (MS) is very rare in industrialized countries and declining in emerging regions is just one reason for that. Balloon-expandable prosthesis designed for TAVI can be implanted into heavily calcified MS or degenerated biological valve prostheses (ViV procedure) restoring physiological diastolic filling of the left ventricle (LV). There is always a risk of LV outflow tract obstruction and must therefore be planned carefully. However, large majority of patients with mitral valve disease shows regurgitation, which finally causes congestion and subsequent left-to-right heart failure. TAVI prostheses, which need calcified environment, cannot be used for therapy of mitral regurgitation (MR). Among numerous percutaneous devices just one implant to be deployed through a transapical approach (no classic percutaneous access) could gain acceptance. That is why, TMVR does not loom large. Instead, surgical and percutaneous mitral valve repair are considered therapeutic approaches of choice.
Other Percutaneous Valve Implantation
As severe tricuspid regurgitation (TR) has been largely undertreated in the past due to questionable surgical results, the first percutaneous tricuspid valve replacement (TTVR) system has been recently approved. However, this therapy is still preserved for life-threatening conditions as is severe and highly symptomatic TR. At present and in near future, majority of patients will undergo percutaneous tricuspid valve repair using similar techniques as proven successfully for treatment of MR. For those who received surgical valve replacement in the past, percutaneous ViV implantation remains an option as described above.
Percutaneous pulmonary valve implantation (PPVI) has been in use for more than two decades to treat patients with pulmonary stenosis, RV hypertension due to dysfunction of the outflow tract after surgical repair of congenital heart disease or, as another ViV procedure, for carriers of surgical valve prostheses.
Percutaneous Valve Repair
Procedures summarized under this term are characterized by targeted changes of valve anatomy in order to mitigate regurgitation and restore valvular function. These techniques are just applicable to non-calcific mitral and tricuspid valves.
Clipping Techniques
Valve clipping has been in use for about fifteen years. Valve leaflets are permanently clipped together what is also known as ‘edge-to-edge repair’, although it does not represent any real repair of the valve. However, ‘clipping’ enables leaflets to better adapt and consequently the valve to close more sufficiently during systole. Therefore, one or more clips are deployed via the inferior vena cava from the left atrium (requires previous septal puncture) to the mitral valve or directly from the right atrium to the tricuspid valve using sophisticated catheter-based delivery systems. The technique can be employed in valve prolapse and in cases of functional regurgitation but is prohibited in valve degeneration due to endocarditis. It is inefficient in cases of leaflet perforation or paravalvular regurgitation.
Annulus Modulation
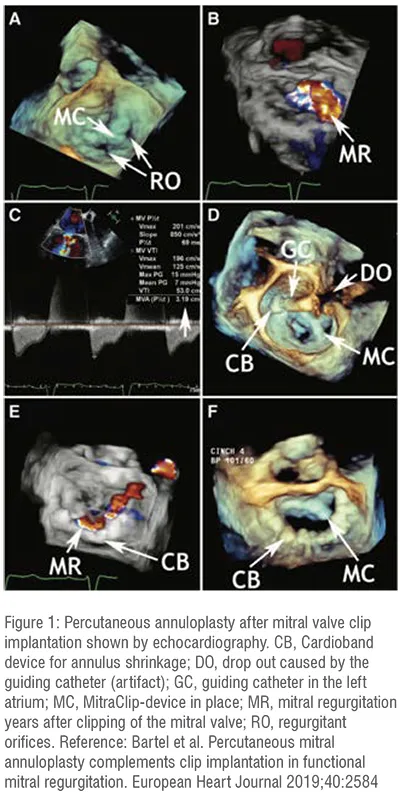
TR and MR are often considered ‘functional’ as a result of annulus dilatation. In these scenarios, percutaneous annuloplasty is an option if a surgical one is too risky. However, these procedures are extremely challenging and are provided just by a few teams worldwide. Devices induce shrinkage of valve annulus from inside the RA or the left atrium (LA). For mitral annuloplasty, devices can be implanted into the coronary sinus for achieving shrinkage from outside the mitral annulus. Percutaneous annuloplasty can also be combined with clipping techniques what may improve sustainability of the result (figure 1).
Percutaneous Devices for Treatment of Congenital Heart Diseases
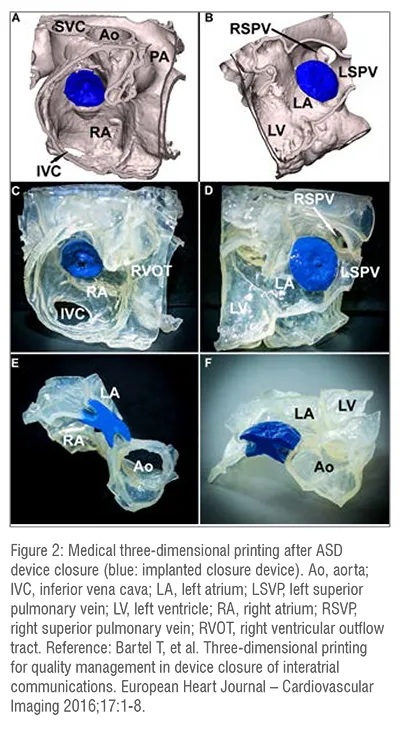
This set of implants has had a kind of pioneering role and initiated the era of catheter-based, permanent deployment of devices. Closure of patent foramen ovale (PFO), atrial septal defect (ASD) and patent ductus arteriosus (PDA) are straightforward procedures performed via a transfemoral venous approach. Most commonly, closure devices consisting of nitinol are released from a tube catheter previously introduced into the opening. Devices each consist of a left-sided and a right-sided counter occlude (figure 2). The left-sided one is released first and closes the opening from the arterial side. The right-sided one is released in a second step and is then pushed against the opening from the venous side. Within six months, devices become permanently ingrown preventing the patient from shunting and paradoxical (venous to arterial) embolism. PFO device closure is explicitly done for secondary prevention of strokes and other arterial embolism. ASD device closure may be indicated if left-to-right shunting causes significant recirculation of blood through the pulmonary vascular tree leading to pulmonary hypertension, right heart overload and finally to impairment of pulmonary function. Stroke prevention has been accepted as another indication. In contrast, PDA device closure is just indicated for interruption of aortopulmonary shunting and therefore, implementation of physiological cardiopulmonary hemodynamics.
Percutaneous Left Atrial Appendage Closure
Left atrial appendage (LAA) device closure is to prevent patients from clot formation inside the LA, which is considered cardiac source of embolism. It is recommended for those individuals suffering from chronic atrial fibrillation (AF) who are no candidates for long-term anticoagulation because of increased bleeding risks, e.g. those with severe bleeding events in history or concomitant diseases, which entail increased likelihood of bleeding. Deployment of dedicated occluder devices is very similar to device closure of interatrial communications or PDA but requires transseptal puncture as mentioned above for clipping of the mitral valve. In LAA closure, devices work as ‘place holders’ to shut the LAA out of circulation. Percutaneous LAA device closure has gained worldwide acceptance for stroke prevention as an effective alternative to long-term anticoagulation in AF.
Non-permanent Cardiac Devices
There are devices for mechanical circulatory support providing long-term or short-term but no permanent assistance to patients with acute or chronic heart failure to keep their heart pumping enough blood, e.g. LV assist devices (LVADs). Such devices are temporarily implanted in order to ‘bridge’ patients to heart transplantation, to gain time for effective drug treatment or to optimally prepare for heart surgery. Intra-aortic balloon pump or intraventricular heart pump are other temporary devices just left inside the human body for a few days to recover from acute left or right heart failure. They are also increasingly in use to support circulation during risky percutaneous procedures, e.g. coronary intervention of the left main stem if LV function is already impaired. Such kind of temporary assistance is prone to improve safety of these procedures.
Health Economical Aspects
Implantation of cardiac devices usually entails high costs. Particularly, percutaneous procedures for device implantation require highly trained and specialized personnel and sophisticated devices are comparatively expansive. In those healthcare systems, settlement is based on diagnoses related groups (DRGs), such procedures are remunerative for health care providers, what finally may end up in some oversupply. In contrast, high costs may prevent patients from receiving adequate therapy in budget-based healthcare systems so that certain undersupply may be a consequence if budgeting is insufficient.
In summary, medical devices are thought to restore or at least improve cardiac functionality. Vast majority of implants just requires minimal invasive or completely percutaneous procedures but no open-heart surgery anymore. With aging of the population, implantable cardiac devices are increasingly in common use.


