How to Maximize Personal Health Records (PHR) Data Utilization: Comprehensive Disease Screening Test Recommendation
Piyanun Yenjit, Founder and Managing Director, APUK Co Ltd.
Periodic health examinations (PHE) are a critical step in disease screening and prevention. However, most people and non-primary care professionals can only list some appropriate investigations. Self-assessment with common information in the Personal Health Records (PHR) application plus advanced medical logic is one solution to getting a comprehensive PHE item.

Disease screening is the process of identifying high-risk patients with specific diseases from the general population. This process for an asymptomatic population differs from early diagnosis, which is suitable for patients with symptoms. Cancer represents a good example to show the several benefits of screening. Here are some examples:
• Reduction in the incidence and mortality of colorectal cancer.
• Less aggressive treatment, e.g., chemotherapy for breast cancer.
• Early-stage treatment also reduces overall healthcare budget spending, according to the health economic perspective.
However, the disease screening programme is not without risk. The most common adverse events resulting from inappropriate screening are false positive and false negative results, over diagnosis, and overtreatment.
• False-positive screening results often lead to unnecessary additional investigation and complication. Aside from that, psychological effects such as depression and anxiety may be discovered. In the healthcare system's management view, this unnecessary intervention may impact other patients' waiting times.
• False negative screening results also lead to delayed diagnosis and treatment. This error may bring liability and reputational risk to the healthcare provider.
• Overdiagnosis and overtreatment: true positive results may not benefit. There are some diseases in which early and late detection make no difference in treatment outcomes. For example, a disease with slow progress.
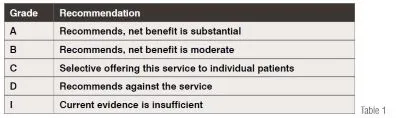
To avoid the above events, selecting screening tests for patients based on evidence-based medicine is essential. Among standard references, the U.S. Preventive Services Task Force (USPSTF) is a reliable and easy-to-use resource for primary care physicians and nurses.
The USPSTF is an independent volunteer panel of national experts in preventive and evidence-based medicine. The Task Force works to improve the health of people nationwide by making evidence-based recommendations about clinical preventive services such as screenings, counseling services, and preventive medications. Task Force members come from the fields of preventive medicine and primary care. The Task Force assigns each recommendation a letter grade based on the strength of the evidence and the balance of benefits and harms of a preventive service.
Although disease screening references are already in place, according to the author's survey of doctors and nurses from one of Newsweek's top 250 world's best hospitals in 2022 with more than ten years of experience in the primary care setting and a screening package that was conducted in February 2023, it shows that all patients were suggested to take at least one unnecessary screening test. Electrocardiograms and tumor markers are the most common unnecessary screening tests.
• Ovarian cancer: The guideline recommends against screening for ovarian cancer in asymptomatic women. This recommendation applies to asymptomatic women who are not known to have a high-risk hereditary cancer syndrome. (Grade D)
• Cardiovascular disease: recommends against screening with resting or exercise electrocardiography (ECG) to prevent cardiovascular disease (CVD) events in asymptomatic adults at low risk of CVD events. (Grade D)
Moreover, the majority of them didn't receive complete guidance on the best screening tests or appropriate screening tests. The five investigations listed below are prioritized in the 55-year-old population based on disease severity and frequency of neglect.
• Osteoporosis: recommends screening for osteoporosis with bone measurement testing to prevent osteoporotic fractures in postmenopausal women younger than 65 years who are at increased risk of osteoporosis, as determined by a formal clinical risk assessment tool. (Grade B)
• Colorectal cancer screening is recommended for all adults aged 50 to 75 (Grade A).
• Breast cancer screening mammography every two years for women aged 50 to 74 years (Grade B).
• Cervical cancer screening is recommended every 3 years for women aged 30 to 65 years, every 5 years for high-risk human papillomavirus (hrHPV) testing alone, or every 5 years for hrHPV testing in combination with cytology (co-testing) (Grade A).
• Lung cancer: The CDC recommends annual screening for lung cancer with low-dose computed tomography (LDCT) in adults aged 50 to 80 years who have a 20-pack-year smoking history and who currently smoke or have quit within the past 15 years. (Grade B)
Common root causes:
• Attitude: Most screening staff suggest screening tests based on age and gender. Only a small portion of the information from the assessment form—which asks about the underlying disease, family history, and lifestyle risk—is used in the analysis. These data are also used to evaluate in some cases. Still, it depends on the screening staff’s experience. Patients usually focus on non-invasive off-label cancer screening investigations, e.g., carcinoembryonic antigen (CEA), alpha-fetoprotein (AFP), etc. Osteoporosis is also overlooked because of the low level of concern in the general population.
• History-taking limitation: As screening is a general health approach, it requires a multi-dimensional history, including a sexual and some health risk history, e.g., illicit drug use. This data is confidential and will take some time to gather and consolidate. The short period of assessment time and taking the assessment in a non-private area are the key barriers to getting a complete history.
• Complexity and variation of screening standards: an indication for some screening tests is not straightforward. Also, there are several steps in the analysis required to get the recommendation. For example, the number of cigarettes smoked per year is required for lung cancer screening recommendations.
• Financial concern: Although colon cancer screening is clearly recommended for adults aged 50–75, some populations may still be prevented from getting the necessary screenings because they lack full financial coverage.
• Test preparation: Some tests require more preparation and more time. For example, a half-day is required for bowel preparation before a colonoscopy.
Solutions:
Giving the patient more time to fill out the data in a suitable format in a private area with a standard medical analysis by an experienced assessor appears to be the best approach to obtaining a screening test list. Unfortunately, this ideal solution requires a lot of resources, especially investments in healthcare staff allocation and training.
Currently, there are many personal health records (PHR) applications or other applications that a user can use to enter necessary personal and medical data for screening test analysis. For example, in health insurance-related applications the required data standard, completeness, and input method are the key challenges for data input. Moreover, there is still room for improvement in terms of analytics features and healthcare provider connectivity. After reviewing 5 personal health record apps with ratings higher than 4 stars in the App Store as of February 23, it was discovered that in all apps, a user is able to input the majority of the necessary data to analyze a personalized screening test. Therefore, comprehensive data input in a comfortable environment (without rushing and in private) is no longer a concerning issue.
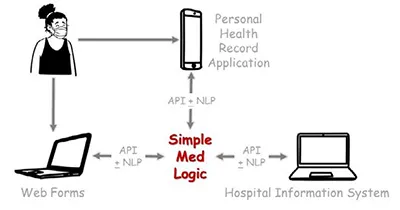
The medical standard microservice is one solution that can be used to analyze screening tests and connect to healthcare providers. Although free-text input is also more useful via the Natural Language Processing (NLP) microservice, Simplemedlogic (SML) is a sample of self-assessment that includes effective medical analysis. Also, even though SML has not yet been connected to any PHR or healthcare provider, it has demonstrated the ability to connect via API, as shown in Figure 1.
Summary
Screening tests provide strong benefits to the general population and the healthcare system. A medical guideline is already in place to prevent adverse events like false negatives and overdiagnosis, but there are some implementation barriers, such as healthcare workers' attitudes, the complexity of the guidelines, and the limitations of a history-taking environment. To achieve excellent disease screening, a complete history review and advanced medical analysis are the key actions. While PHR is used for data input, medical microservice plug-ins can also be the solution for better analysis. This combination will make health screening more complete and affordable.
Author Bio

Piyanun Yenjit is the HIMSS Thailand country manager and founder of APUK, a healthcare digital transformation consultant and microservices provider, focusing on improvement in patient safety, process efficiency, and business growth. She is also experienced in electronic medical records with structured data implementation compatible with various quality assurance standards.

